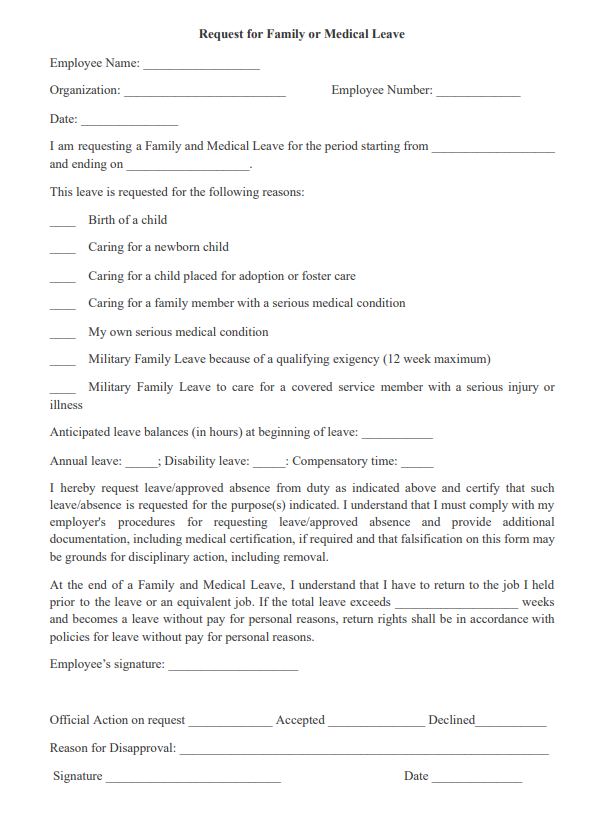
This Request for Family or Medical Leave is from an employee to an employer in order to request time off as a family or medical leave. This request sets out the name of the employee, the start and end dates of the leave and the specific reason why leave is being requested.
The composition of families in the United States has changed significantly in the past few decades. A major legal requirement regarding family-oriented benefits is the Family and Medical Leave Act (FMLA), which provides for unpaid leaves of absence.
The Family and Medical Leave Act of 1993 (FMLA) is a United States labor law requiring covered employers to provide employees with job-protected and unpaid leave for qualified medical and family reasons. The FMLA was enacted in 1993 and has been amended several times. It covers all federal, state, and private employers with 50 or more employees who live within 75 miles of the workplace.
Only employees who have worked at least 12 months and 1,250 hours in the previous year are eligible for leave under the FMLA. The law provides for unpaid leave; however, some companies pay short-term disability benefits during FMLA leaves under certain conditions.
A serious health condition is an illness or injury that requires inpatient care or continuing treatment by a health care provider for medical problems that exist beyond three days. An employer may require a medical certificate from a health care provider to support the reason for the employee’s leave.
Since the enactment of the FMLA, a significant percentage of employees have taken family and medical leave.
Related Forms:
Other Forms
- Affidavit Forms
- Assignment Forms
- Attorney Forms
- Bankruptcy Forms
- Bill of Sales Forms
- Borrow, Lend & Collection Forms
- Business Forms
- Confidentially Forms
- Contract Forms
- Copyright Forms
- Corporation Forms
- Credit Form
- Declaration Form
- Deed Forms
- Divorce Forms
- Employment Forms
- Entertainment Contract Forms
- Family Law Forms
- Free Will Forms
- Government Form
- Health Care Forms
- Homestead Form
- Indemnity Agreement Form
- Intellectual Property Forms
- Internet Forms
- Landlord and Tenant Forms
- Lease and Rental Forms
- Letter Forms
- Limited Liability Co. Form
- Non-Compete Forms
- Non-Disclosure Forms
- Notice Forms
- Parental Permission Forms
- Partnership Forms
- Power of Attorney Forms
- Premarital Forms
- Promissory Notes
- Real State Forms
- Release Forms
- Sale & Purchase Forms
- Technology Forms
- Trademarks Forms
- UCC Forms